
ISSUE1741
- Mark Abramowicz, M.D., President has disclosed no relevant financial relationships.
- Jean-Marie Pflomm, Pharm.D., Editor in Chief has disclosed no relevant financial relationships.
- Review the American College of Cardiology/American Heart Association recommendations for primary aldosteronism screening in patients with hypertension.
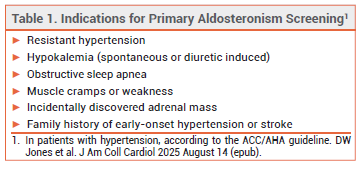
Recently published guidelines recommend screening patients with hypertension for primary aldosteronism. The Endocrine Society recommends screening all patients1 and the American College of Cardiology/American Heart Association (ACC/AHA) recommend screening those at increased risk (see Table 1).2
PRIMARY ALDOSTERONISM — Primary aldosteronism is the most common cause of secondary hypertension. It affects up to 20% of patients with resistant hypertension and is associated with an increased risk of cardiovascular morbidity and mortality compared to primary hypertension. Overproduction of aldosterone with low plasma renin leads to increased sodium levels, water retention, and decreased potassium levels.3
SCREENING — Screening for primary aldosteronism includes measuring plasma aldosterone levels and plasma renin activity to determine the aldosterone to renin ratio (ARR). If hypokalemia is present, screening should be repeated after it is corrected. Mineralocorticoid receptor antagonists (MRAs) such as spironolactone and eplerenone should be discontinued at least 4 weeks before screening. The ACC/AHA guideline recommends continuing most other antihypertensive drugs during screening.2
TREATMENT — Targeted treatment of primary aldosteronism is associated with improved kidney and cardiovascular outcomes. The treatment of choice in patients with unilateral aldosterone overproduction is unilateral adrenalectomy; in patients who have bilateral overproduction or are not candidates for surgery, the treatment of choice is an MRA. Clinical trials of aldosterone synthase inhibitors (e.g., baxdrostat, lorundrostat) are ongoing.
- GK Adler et al. Primary aldosteronism: an Endocrine Society clinical practice guideline. J Clin Endocrinol Metab 2025; 110:2543. doi:10.1210/clinem/dgaf284
- DW Jones et al. 2025 AHA/ACC/AANP/AAPA/ABC/ACCP/ACPM/AGS/AMA/ASPC/NMA/PCNA/SGIM guideline for the prevention, detection, evaluation, and management of high blood pressure in adults: a report of the American College of Cardiology/American Heart Association Joint Committee on clinical practice guidelines. J Am Coll Cardiol 2025 August 14 (epub). doi:10.1016/j.jacc.2025.05.007
- JB Byrd et al. Primary aldosteronism: practical approach to diagnosis and management. Circulation 2018; 138:823. doi:10.1161/circulationaha.118.033597